[VIDEO with 39 SLIDES] – Dr. Rebecca Shatsky, MD from the 2024 MOASC Annual Oncology Summit & Research Symposium
In the rapidly advancing field of breast cancer treatment, the emphasis on personalizing therapy to individual patient needs and tumor characteristics has become increasingly paramount. Dr. Rebecca Shatsky, MD an esteemed Associate Professor of Clinical Medicine at UC San Diego, provides an in-depth exploration of the latest strategies and breakthroughs in breast cancer management at the 2024 MOASC Annual Oncology Summit & Research Symposium. This article delves into the critical aspects of her presentation, which spans the gamut from the nuanced application of chemotherapy in HR+/HER2- early breast cancer (EBC) to the cutting-edge advancements in adjuvant targeted therapy, and from the evolving landscape of early HER2-positive and triple-negative breast cancer (TNBC) to the complexities of treating metastatic breast cancer (MBC).
Determining Chemotherapy Necessity in HR+/HER2- Early Breast Cancer
A pivotal aspect of treating HR+/HER2- EBC involves discerning which patients stand to benefit from chemotherapy. Dr. Shatsky emphasizes the role of genomic assays, such as Oncotype DX and Mammaprint, in informing these decisions. The utilization of these assays in patients with node-negative disease and those with 1-3 positive lymph nodes can significantly impact treatment choices, underscoring the value of precision medicine in this context. The RxPONDER trial, in particular, brings to light the varied chemotherapy benefits across different menopausal statuses, advocating for a personalized approach to therapy.
Optimizing Endocrine Therapy
Endocrine therapy is a cornerstone in managing HR+/HER2- breast cancer, with choices extending between tamoxifen and aromatase inhibitors, supplemented by considerations for ovarian function suppression in premenopausal women. The nuanced decisions regarding the type and duration of endocrine therapy are informed by trials such as SOFT/TEXT and POSITIVE, which shed light on the optimal use of these therapies. The question of extending endocrine therapy beyond the initial five years is addressed through both clinical assessments and genomic tools like the Breast Cancer Index, highlighting the move towards more individualized treatment plans based on the patient’s risk assessment.
Advancements in Adjuvant Targeted Therapy
The advent of CDK4/6 inhibitors like abemaciclib and ribociclib in the adjuvant setting for patients with high-risk HR+/HER2- EBC marks a significant evolution in breast cancer treatment. The MONARCHE and NATALEE trials not only demonstrate the efficacy of these agents in improving invasive disease-free survival but also signify their role in enhancing standard endocrine therapy. Additionally, the OLYMPIA trial underscores the importance of PARP inhibitors, such as olaparib, for patients with germline BRCA1/2 mutations, further stressing the necessity of genetic testing in guiding therapy selection.
Updates in Early HER2+ and TNBC Management
In early-stage HER2-positive breast cancer, the TRAIN-2 trial evaluates the necessity of anthracyclines when dual HER2 blockade is employed, indicating high pCR rates can be achieved without their use. For TNBC, a challenging and aggressive subtype, the KEYNOTE-522 trial illustrates the potential of pembrolizumab in augmenting event-free survival, marking a significant step towards integrating immunotherapy into standard treatment regimens.
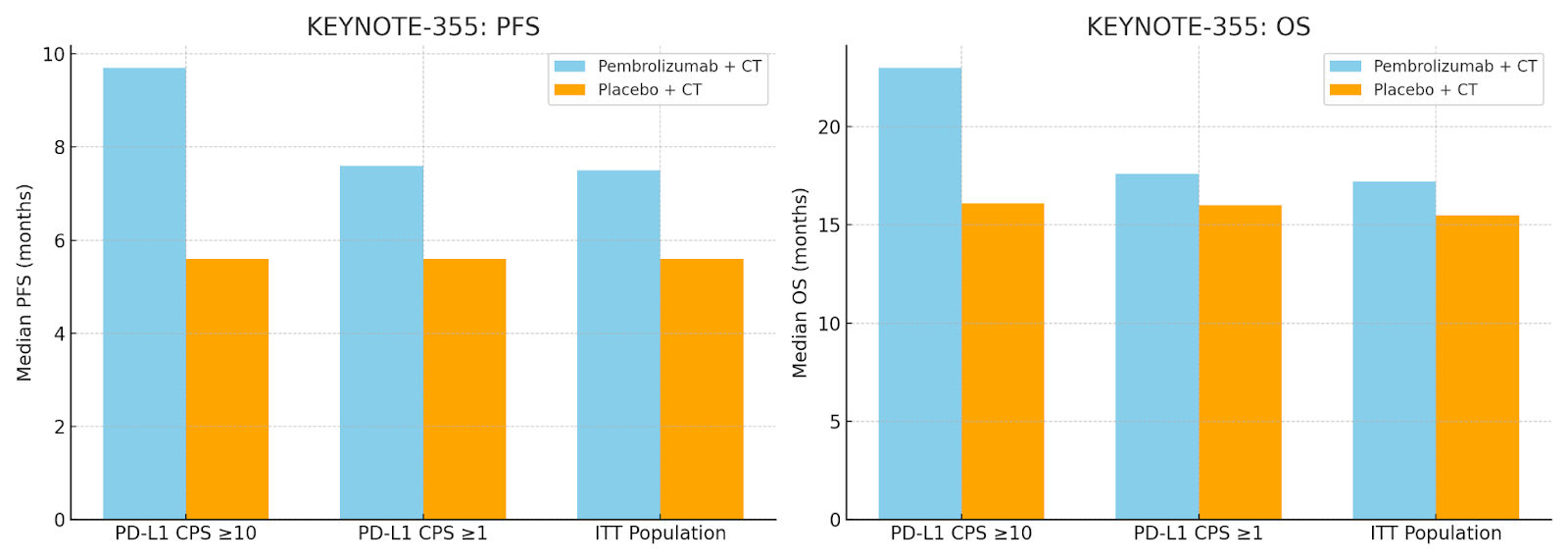
Graph for the KEYNOTE-355 trial showcasing the median progression-free survival (PFS) and a simulated overall survival (OS) comparison between the Pembrolizumab + Chemotherapy (CT) group and the Placebo + CT group. These visualizations highlight the differences in median PFS and a hypothetical OS across various PD-L1 CPS categories and the ITT population, illustrating the impact of Pembrolizumab treatment in enhancing patient outcomes.
Navigating the Treatment of Metastatic Breast Cancer
Treating MBC requires a deep understanding of the disease’s molecular underpinnings. The ASCO guidelines recommend testing for PIK3CA mutations to identify candidates for alpelisib plus fulvestrant. The evolving SERD landscape, exemplified by the success of agents like elacestrant in the EMERALD trial, opens new avenues for targeting ER+/HER2- MBC with ESR1 mutations. The efficacy of sacituzumab govitecan in TNBC and T-DXd in HER2-low breast cancer highlights the expanding therapeutic options available for MBC, demonstrating the ongoing efforts to enhance treatment efficacy and patient outcomes.
Conclusion
The path towards personalized breast cancer treatment is marked by continuous research and innovation. Dr. Shatsky’s comprehensive overview illuminates the critical advancements in the field, from the judicious use of chemotherapy and endocrine therapy in early-stage disease to the application of novel targeted therapies in both early-stage and metastatic settings. As the breast cancer treatment landscape evolves, oncologists are equipped with a growing array of tools to tailor treatments to individual patient needs, aiming to improve outcomes and enhance the quality of life for those affected by this complex disease.
Reference Links:
Study of Pembrolizumab (MK-3475) Plus Chemotherapy vs. Placebo Plus Chemotherapy for Previously Untreated Locally Recurrent Inoperable or Metastatic Triple Negative Breast Cancer (MK-3475-355/KEYNOTE-355): https://clinicaltrials.gov/study/NCT02819518
OncologyTube Links:
NATALEE Trial ESMO 2023: Guideline Changes?: https://oncologytube.com/natalee-trial-esmo-2023-guideline-changes/