Introduction to ADCs in Cancer Therapy
The advent of targeted therapies has revolutionized the field of oncology, offering new hope and improved outcomes for patients with hematological malignancies. Among these innovative treatments, Antibody-Drug Conjugates (ADCs) such as Inotuzumab Ozogamicin (INO) and Gemtuzumab Ozogamicin (GO) have emerged as significant advancements. These therapies uniquely combine the specificity of monoclonal antibodies with the potent cytotoxicity of chemotherapeutic agents, specifically targeting cancer cells while sparing healthy tissue. However, the clinical application of INO and GO has unveiled a challenging aspect of their use: liver toxicity, including sinusoidal obstruction syndrome (SOS) and thrombocytopenia. Drawing on the work of Dr. Mojtaba Akhtari, MD, FACP, this article delves into the mechanisms behind this toxicity, its clinical presentation, and strategies for management, offering a comprehensive guide for oncologists.
Detailed Background on INO and GO Mechanisms
INO and GO represent a class of ADCs that target antigens expressed on the surface of leukemia cells. INO is directed against CD22 on B-cell Acute Lymphoblastic Leukemia (B-ALL) cells, while GO targets CD33 on Acute Myeloid Leukemia (AML) cells. The shared cytotoxic agent between them, calicheamicin, is a potent chemotherapy that causes double-stranded DNA breaks, leading to cell death. Despite their targeted action, these drugs can induce severe liver toxicity, manifesting as SOS and thrombocytopenia, which poses significant risks to patients.
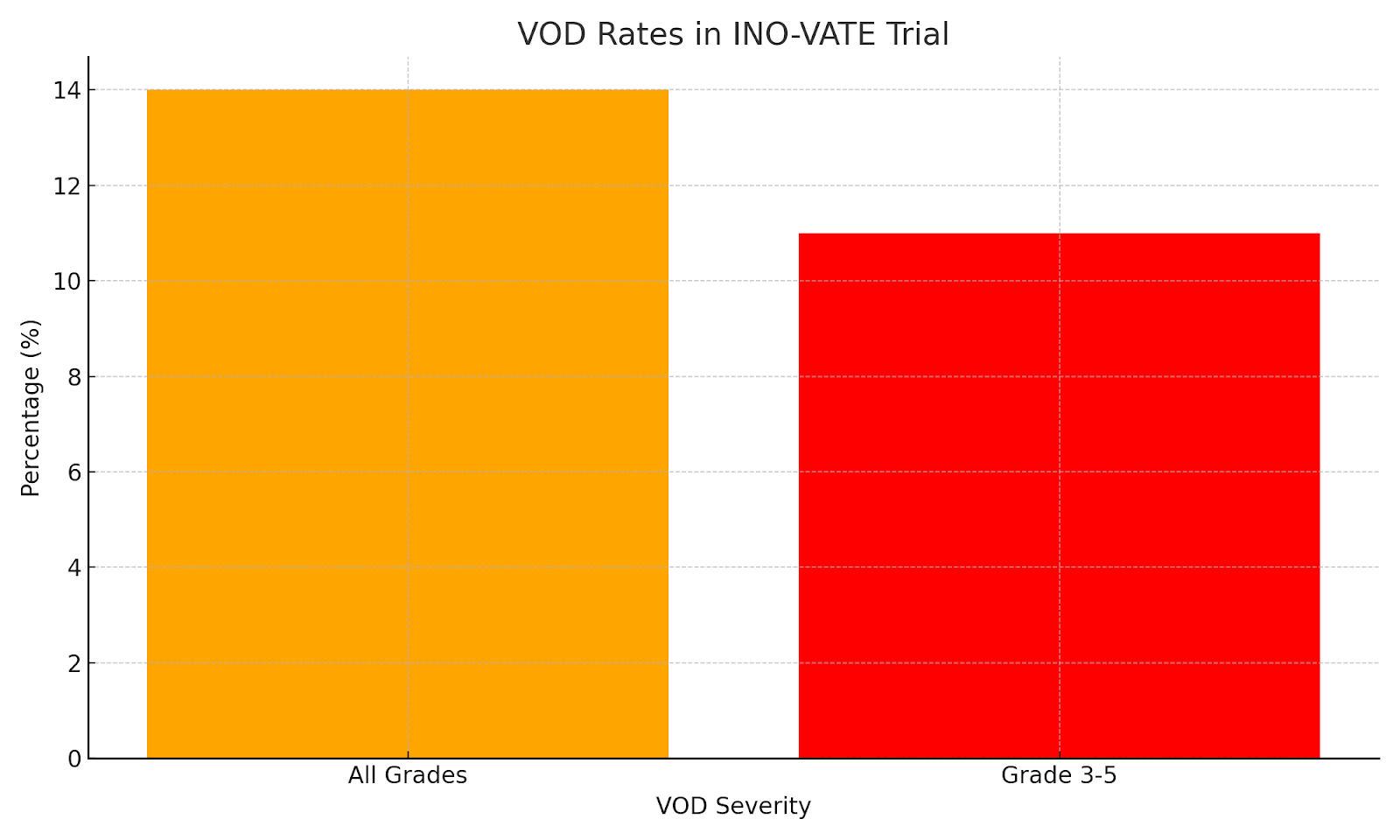
VOD Rates in INO-VATE Trial: This graph displays the percentages of patients experiencing VOD of all grades versus grades 3-5 in the INO-VATE trial, indicating the severity of liver toxicity.
Clinical Presentation and Case Studies
The liver toxicity associated with INO and GO can range from mild, characterized by elevated liver enzymes, to severe, presenting as hepatomegaly, portal hypertension, and even encephalopathy. Dr. Akhtari’s clinical observations provide insight into this spectrum of hepatotoxic effects. For instance, five patients with relapsed/refractory B-ALL exhibited elevated liver function tests (LFTs) and abnormal liver imaging after receiving INO. While symptoms and signs resolved in four patients after pausing INO, one patient succumbed to progressive liver disease, highlighting the variable clinical course and the potential for fatal outcomes.
Pathophysiological Insights into ADC-Induced Liver Injury
The mechanism of liver toxicity from INO and GO involves the disruption of the sinusoidal endothelial cell barrier and damage to hepatocytes within the liver’s acinus. Calicheamicin, upon being released into the target cells, not only destroys the cancer cells but also affects the surrounding liver tissue. This damage leads to gaps in the sinusoidal barrier, allowing cells and debris to accumulate in the space of Disse, subsequently causing venous lumen narrowing, post-sinusoidal portal hypertension, and centrilobular hemorrhagic necrosis. Understanding this pathophysiology is crucial for oncologists to anticipate and recognize the early signs of liver toxicity in their patients.
Management Strategies and Preventive Measures
The management of liver toxicity in patients receiving INO and GO requires a multifaceted approach. Oncologists should exercise caution by avoiding additional hepatotoxic drugs and limiting the treatment cycles of INO, particularly in candidates for Allo HSCT. Regular monitoring for symptoms and laboratory indicators of liver injury is imperative for early detection and intervention. The prophylactic administration of Ursodeoxycholic acid is recommended for all patients, irrespective of their eligibility for Allo HSCT, to mitigate the risk of hepatotoxicity. Additionally, the decision between initiating treatment with INO or Blinatumomab (BLIN) should be personalized, considering the patient’s overall medical condition and the potential toxicity of each drug.
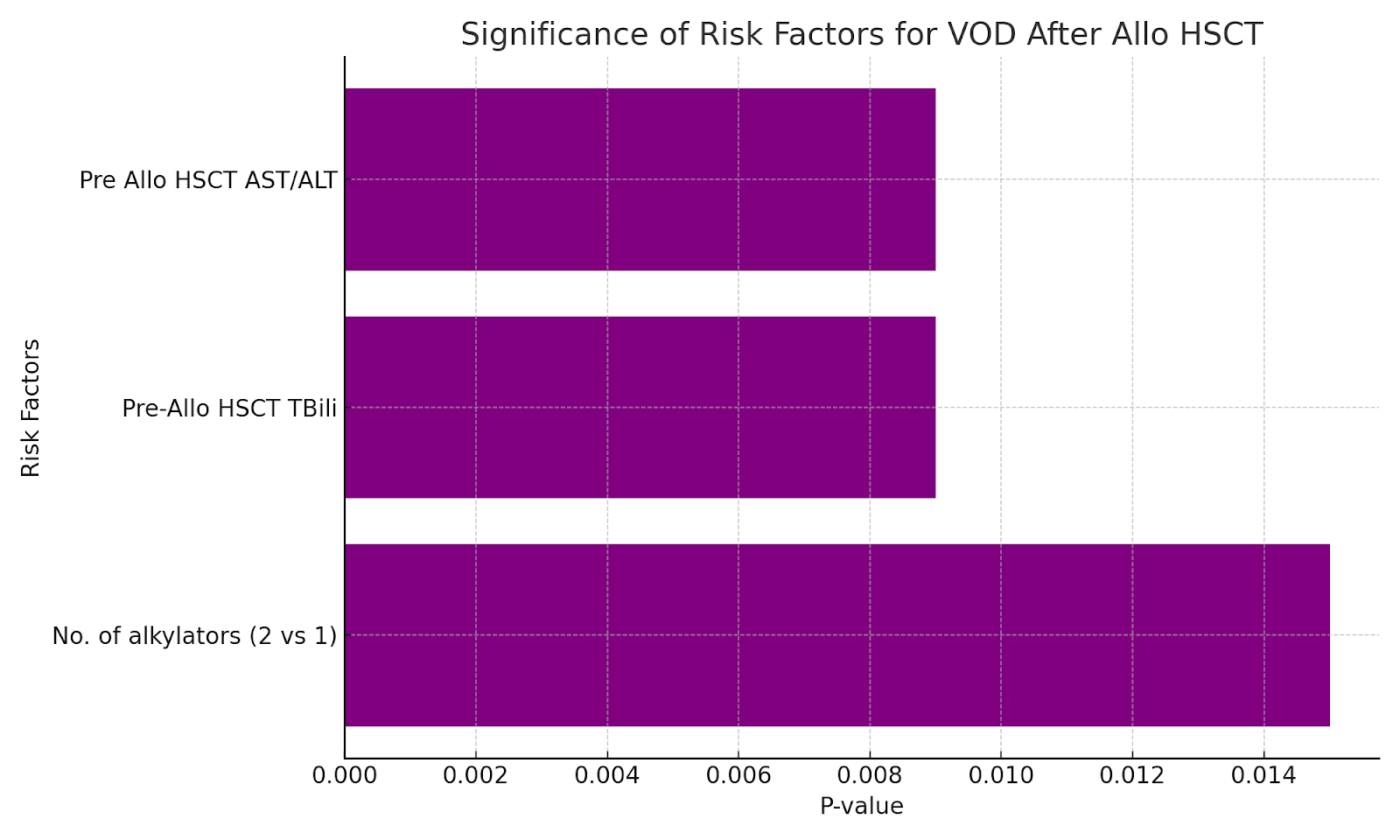
Significance of Risk Factors for VOD After Allo HSCT: A bar graph showing the p-values for significant risk factors for VOD after Allo HSCT, illustrating the statistical significance of each factor.
A Holistic View on Patient Care and Acknowledgements
The management of liver toxicity induced by ADCs underscores the importance of a comprehensive and patient-centered approach to cancer care. Oncologists play a critical role in navigating these complexities, balancing the benefits of these potent therapies against their risks. The dedication of cancer patients, their families, and the broader healthcare team, including nurses, pharmacists, and support staff, is central to achieving the best possible outcomes. This collaborative effort embodies the spirit of the saying, “Whoever Saves a Life Saves the World,” highlighting the collective endeavor to advance cancer treatment while ensuring patient safety.
Concluding Remarks on ADC Therapy in Oncology
INO and GO offer promising avenues for the treatment of hematological malignancies, representing the cutting edge of personalized cancer therapy. However, their potential for inducing liver toxicity necessitates vigilance and a proactive management approach from oncologists. By deepening our understanding of the underlying mechanisms, risk factors, and effective prevention and treatment strategies, the oncology community can optimize the therapeutic potential of ADCs. This comprehensive approach will not
Reference Links:
LiverTox: Clinical and Research Information on Drug-Induced Liver Injury: https://www.ncbi.nlm.nih.gov/books/NBK547906/
OncologyTube Links:
FDA Approves Inotuzumab Ozogamicin (BESPONSA) for Acute Lymphoblastic Leukemia in Pediatric Patients: https://oncologytube.com/fda-approves-inotuzumab-ozogamicin-for-acute-lymphoblastic-leukemia-in-pediatric-patients-exclusive-video/