


Belzutifan and other Novel Therapies in Genitourinary Oncology 2023
By Rana McKay, MD – University of California San Diego
We’re gonna start with kidney cancer and go through Belzutifan, Relatlimab, SRF-388 and the others that are listed here. Then we’ll go into. And finally urothelial cancer. This is gonna be a little bit of a whirlwind, splash on each of these drugs where they’re at. And then tie it all up at the end.
Renal Cell Carcinoma 2023 Update
So we’ll start with kidney cancer and first we’ll talk about Belzutifan. and it’s, I have to say it’s been amazing taking care of kidney cancer patients and seeing the evolution of the treatment of this disease over the last decade because all of the drugs that we have to treat kidney cancer, We’re based on Nobel prize level work, which is pretty quite remarkable. So we all know that in states of hypoxia or pseudo hypoxia, where a vhl gene is, mutated, h accumulates in the cell and actually results in angiogenesis and proliferation. and, Belzutifan is a small molecule inhibitor of, H two Alpha. these are the data from the LITESPARK-001 – Phase 1 trial.
This was a trial that was conducted in heavily pretreated clear cell RCC patients. There were 55 patients that were enrolled on the trial. The median number of lines of prior therapy was three, and you could see that the objective response rate was 25%. The progression-free survival. 14.5 months, and there’s currently a large Phase 3 that’s looking at the role of Belzutifan in the refractory setting in RCC.
This trial has completed accrual and we are all eagerly awaiting the results. Belzutifan already has an approval in kidney cancer for patients with vhl-. so associated disease, hereditary via cell. , but not yet for sporadic disease. There are other studies that are looking at Belzutifan in other combinations. There’s LITESPARK-003, which looks at Belzutifan in combination with Cabozantinib.
Associated Renal Cell Carcinoma
There were two cohorts that enrolled onto this trial cohort. One was for treating naive patients. doing. Belzutifan with Cabozantinib and the Belzutifan dosing was at one 20 and Cabozantinib dosing was at 60. In the context of this clinical trial however, they have different, slightly different mechanisms of action with regards to their toxicity profile, you don’t get that t k I talks with the Belzutifan. It’s mainly anemia and shortness of breath. And then cohort two was in prior IO treated patients. And we can see top line data here for cohort one. That was the treatment Naive again was 57%. Cohort two was 31. this trial is continuing to accrue patients and so I think, you know, we’ll see about different combination strategies in, RCC.
So there’s a frontline trial Merck 012, that’s also accruing patients. we’ve heard some data at the, early, late last year about cosmic 313, which looked like triple therapy. In metastatic RCC, there are other triple therapy combinations that are being explored. This trial uses the backbone of lenvatinib and pembrolizumab and then adds to.
Bone Belzutifan, so triple of Len Belzutifan and then LePen plus CTLA four inhibition. So that trial is currently ongoing and there’s also another trial looking at Belzutifan lenvatinib in the second line setting that’s also occurring. And so I, I, I actually think that one may have near completed accrual, but, so these are additional studies of Belzutifan.
I think this is probably the next kit on the block if I had to guess renal cell carcinomas. So, a very exciting agent. All right. We’ll talk about the different strategies to target the immune microenvironment. So there’s stimulatory and inhibitory immune checkpoints. There’s novel cytokine based therapies to activate T-cell response.
There’s also targeting of immune metabolic pathways. so there’s a lot of interesting and novel IO based treatments to be explored. We’ll talk a little bit about which, we all are familiar with the data in melanoma. This was a phase 2/3 study, double blind randomized trial previously unresected Or, previously, untreated unresected melanoma with a primary endpoint of, PFS.
Combination of Relatlimab plus nivolumab versus nivolumab alone
This trial looked at the combination of Relatlimab plus nivolumab versus nivolumab alone was a positive study leading to an FDA approval of this agent. There is a, study called Fraction RCC, which is a multi-arm open-label trial looking at various IO combinations in. RCC and, and Relatlimab is being explored in that context we don’t actually have any data yet, and I failed to highlight. Relatlimab is a first in class, basically lag three inhibitor that basically restores the effect function of exhausted cells. And so I think this is potentially another promising compound in RCC we’ll talk about SRF-388. SRF-388 is a first in class anti IL-27 antibody.
We know that the immune regulatory cytokine IL-27 upregulates inhibitory immune checkpoint receptors such as PD-l1, and then downstream proinflammatory cytokines. There is a Phase 1 trial that’s currently ongoing, a Phase 1 first in hand with this agent. There’s been some, there’s multiple, That are enrolling on that study, but a little bit of a signal of some activity in the clear cell RCC dose expansion.
A hundred percent of patients had received prior IO and prior VEGF targeted therapy. And see some early signals of activity. So look for this agent. . And then, the other agent I wanted to highlight is ds, 6,000 a. this is a drug being made by Daichi Sanko, and I have to say there’s a lot of excitement around there.
Cadherin 6
MADC pipeline. so this is a Cadherin 6 directed ADC, with three components. basically the monoclonal antibody that targets, CDH-6 and then your, cleavable linker. And then the payload here is a topo one inhibitor. . so Cadherin 6 is involved in cell cell adhesion and epithelial mesenchymal transition.
Cadherin 6 is overexpressed in RCC and preclinical studies have demonstrated that its inhibition can lead to tor regression. And so this compound is directed, right at this, target. And there’s a Phase 1 study currently ongoing in RCC and ovarian. With some, again, early, very early preclinical data.
GU ASCO 2022
This is data that were presented at ASCO last year, and hopefully we’ll continue to see updated data about this compound. . So I wanna talk a little bit about CA-9 and, we saw some data at GU ASCO just a couple of weeks ago that were presented regarding, imaging, with CA-9 with basically Ziron, Girentuximab.
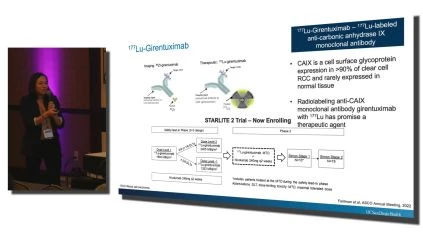
There’s also a therapeutic agent as well that is in testing. So CA-9 is a cell surface transmembrane protein that’s actually. Hypoxia and it’s overexpressed in about 90% of clear cell RCCs and hypoxia and, and vhl laws can actually up-regulate CA-9 expression. It’s very minimally expressed in normal tissue.
Ziron Trial
And, you know, it’s expression can basically well, it’s, it’s expression, like I said, is upregulated by hypoxia. . So J Rituximab is a monoclonal antibody that basically binds to CA-9 and it’s demonstrated safety in prior imaging and therapeutic studies. It’s excreted through the hepatobiliary system and when it’s linked to a zirconi payload, It can actually function like an imaging agent, you can imagine the zirconi. So this was a Phase 3 Ziron Trial including 3000 patients demonstrating increased specificity and sensitivity for actual detection of small renal masses and being able to designate them as actually being, clear cell RCC. Now what’s interesting is actually there’s, you can, link the rituximab to Luteti and then it can actually function as a therapeutic agent, not just an imaging agent. And there are, two studies that are actually currently ongoing here. I just highlighted. STARLITE 2. but, there’s two studies that are currently ongoing with this agent given in combination with nivolumab in the second line setting and nivolumab Cabozantinib in the frontline setting, so I think that we’re gonna see more about, rituximab, and its activity. There was previously some very old data that was presented like almost five or six years ago of rituximab and maybe Monty Pal, MD remembers the very old. Study that tested adjuvant during rituximab that just basically shut down.
But I, you know, I think that the dosing and, safety has been worked out and I think this is something to be. , thinking about in the future, and I always get excited about the imaging here because, you know, you could imagine the role of, of more specific pet imaging tracer in the surveillance setting, for patients with, high risk of disease progression post nephrectomy, and, and, and could RCC evolve into an era like, like prostate cancer. I don. We’ll see. All right, palbociclib. So palbociclib, you’re probably familiar with it, since selective inhibitor of the Cyclin-dependent kinase 46, we know that the CDK 46 are canonically involved in, cell cycle, checkpoint control and dysregulation actually, may and they’re, they play have a dysregulated role in RCC and they could potentially serve as a therapeutic target.
Bill Kalan, MD and others
There’s been some very elegant work that’s been conducted by Bill Kalan, MD and his group, regarding the role of, CDK 4/6 in, inducing Lethal CDK 46 inhibition. In inducing synthetic lethality in RCC cell lines, specifically in vhl loss, models. And there’s a phase two that’s currently ongoing looking at palbociclib in combination with exit and nivolumab, for frontline, RCC, so more to come on the role of CDK4/6 inhibition and, and renal cell carcinomas, but certainly interesting. All right. So now we’re gonna talk about prostate cancer. a lot of interesting targets in prostate cancer. A lot of interesting drugs. this is just like the tip of the iceberg of all the novel drugs that I think are.
Advanced Renal Cell Carcinoma
Being, looked at in prostate cancer. So just bear with me. so first we’re gonna start with, continued targeting of the androgen receptor. So we know that ar alterations continue to be pretty relevant for people who have advanced disease, even in the setting of metastatic castration resistant disease, with regards to the genomic alterations that are seen, we can see ar amplifications in about 60% of individuals with metastatic castration. Resistant disease. There are splice variants where you basically lose the ligand binding domain and have a constituently activated androgen receptor. There’s also AR mutations, and depending on the mutation that’s, seen, there can be promiscuity of the different ligands binding to those muta, that receptors.
So whether it be, you know progesterone or steroids or so forth, . And there’s also potentially alternate ways of blocking testosterone. Here you can see that, we’re all familiar with abiraterone, which is a C 17 liaise inhibitor, but you can actually block further upstream, in the pathway, and we’ll talk about some of those strategies to be able to do that.
ARV-110
So, ARV-110 is a basically a prota, it’s an androgen receptor degrader. It basically helps with targeting the androgen receptor ubiquitin it and basically degrading it in the proteasome. And there’s been some very interesting data that’s been presented about the activity of this agent, particularly in patients who have.
Antigen receptor, mutations and post-progression on drugs like abiraterone and enzalutamide. So there’s some excitement around this cuz this is an unmet need in, in treating metastatic CRPC. You can see here this very elegant three phase preclinical study that was conducted where they treated patients with abiraterone with the ARV-110 and then, they were just treated with abiraterone alone, and then the drug was reinstituted. And you can see in that Phase 3 section where there was real activity of, you know, efficacy, post-progression on these agents. . The other drug to highlight is ODM 208. This is a non-steroidal selective C 11 a inhibitor that actually blocks pretty high up with regards to steroidal production, androgen production, and mineralocorticoid production within the adrenal gland.
And so when it’s given, it’s actually given mineralocorticoids and. Steroids as well, cuz you’re replacing, loss from the inhibition. There was a phase two study that was conducted specifically in men with metastatic CRPC, having received a prior A R S I and a prior taxane. And you can see here,, there was a significant reduction in , You know, psa, that this is the PSA response waterfall pot.
It was like 53%, PSA 50 rates, which is pretty impressive. And all patients that actually had ar ligand binding domain mutations seem to have a response to therapy. The resistance response was 26%. You can also see the corresponding drops in cortisol, and Stein Dion. I think those are the. You know, this is basically inducing adrenal insufficiency, you know, in, in, the highest order, if you will.
Abemaciclib
So other drugs that are being tested in prostate cancer are abemaciclib. Abemaciclib is an oral CDK4/6 inhibitor that also has some activity at CDK nine. This agent is approved across the continu for patients with, ER positive breast cancer. . And then there’s actually three studies that have been ongoing of abemaciclib in prostate cancer building on some very early preclinical work that you can see highlighted here from Karen Knudson’s group and others, the Cyclone one study is looking at a very treatment refractory population of Abemaciclib as a monotherapy Cyclone 2 was, Basically, a phase two three study looking at abemaciclib with abiraterone in the frontline MCRPC study in patients that had never received a prior A R S I and Cyclone 3.
That study has completed accrual and hopefully we will be seeing results in the future. Cyclone 3 is a first line study being conducted in the metastatic hormone sensitive setting for patients with high risk disease where patients are randomized to Aira. Or placebo versus abiraterone and abemaciclib, and that study is currently ongoing.
Capivasertib
The next drug that I’ll highlight is Capivasertib. This is a potent selective, a t p competitive inhibitor of all three AKT isoforms. There is a study that was published called the PROCAID Trial which looked at the combination of this agent with docetaxel and MCRPC and there did seem to be a signal of activity.
There’s currently a large phase three study that’s ongoing. Frontline setting, looking at this agent in combination with abiraterone for patients with metastatic hormone sensitive disease. were familiar with the data regarding IPA AER in the metastatic CRPC setting. That study, you know, met its primary endpoint of PFS but was quite a toxic regimen and, and there was no signal of overall survival. And so, the EPA aib development has been halted in, prostate cancer research now. So we’ll have to see sort of, how Capivasertib AIB pans out what happens with this study. And then DS seven 30. So this is a very exciting compound that I have a lot of excitement about.
I think, again, building on the ADC model of Daichi Sanko. this is ADC, with a payload that targets B seven H three, and B seven. H three is highly expressed in prostate cancer and up other epithelial tors. it’s in the same class of, receptors as actually pd. Suspected to function as a checkpoint, but we don’t know what it does. But nonetheless, it’s a highly expressed agent in, in advanced prostate cancer. and even in hormone sensitive disease, I should say. but this is basically an ADC. , targeting, B seven H three, and there was some early preclinical or early data presented from the Phase 1 study last year at ASCO demonstrating p s a response and objective responses of this agent.
And so I think we’re gonna have to see sort of what happens with it over time.
Prostate Specimen Membrane Antigen
All right. We can’t have a prostate talk without talking about Prostate Specimen Membrane Antigen . I was gonna include some information about Prostate Specimen Membrane Antigen with kidney cancer, but I was not gonna have enough time. But Prostate Specimen Membrane Antigen , is a trans-membrane carboxypeptidase. It’s highly expressed in prostate cancer. and particularly, Static lesions, you know, it’s more so restricted, restricted , expression within normal tissue, it’s an excellent target for pet imaging. . we’ve seen the data for, from the vision trial of, Lutetium Prostate Specimen Membrane Antigen which is a beta emitting, you know, radioisotope that’s linked to the small molecule inhibitor, Prostate Specimen Membrane Antigen . There are other Prostate Specimen Membrane Antigen targeting compounds that are up there. This is the Lu-PNT2002 radiolabeled Prostate Specimen Membrane Antigen targeted small molecule inhibitor.
Splash Trial
This is the splash trial. It’s a large Phase 3 that’s currently ongoing and there’s probably gonna be another me too you know, agents to , target PSMA. . And then, J N J oh eight one is a bispecific antibody that’s binding Prostate Specimen Membrane Antigen and also CD three on T-cells. And there’s a Phase 1 currently ongoing in dose escalation, and expansion with some early preclinical data, looking at, maxim PSA change and, it’s interesting cuz this reg, this agent can be given subcutaneously or can be given intravenously and it almost seems to have a better, pharmacologic efficacy profile when given subq as opposed to given, intravenously. which is interesting. All right, so lastly, we’ll talk about urothelial carcinoma, we’re gonna talk about the Enfortumab vedotin + pembrolizumab data. We’ll talk about Trastuzumab, Cabozantinib and . N-803. So Enfortumab vedotin is an antibody drug conjugate that targets nuttin four with a linker to an MMAAE payload. that’s actually already FDA approved for the treatment of patients with, refractory urothelial carcinoma.
Enfortumab vedotin + pembrolizumab versus Enfortumab vedotin alone
We’ve seen some pretty exciting data about the combination of this agent when given with pembrolizumab. There was a large study large Phase 1 two studies. EV-103, which looked at this combination and in cohort K patients were randomized to Enfortumab vedotin + pembrolizumab versus Enfortumab vedotin alone. not with an intent to compare between those two, allocations, but rather to understand, how Enfortab vedotin is performing in a cis ineligible frontline population and how the combination is performing.
The top line data were presented. ESMO last year, and we saw tremendous responses. you know, over 60% response rate that seemed to happen independent of lectin expression. Over 86% of bladder cancer tors have lectin expression. The 12 month PFS here was at 55.1. this regimen is, Not to say so active, but you know, it takes a lot to challenge cisplatin in the frontline setting in, in bladder cancer.
Cisplatin has been sitting on the throne for a long time as a, as a, you know, very highly effective agent for advanced. bladder cancer, but there’s actually a large Phase 3 trial currently ongoing called Enfortumab vedotin 302. That’s randomizing patients who to cisplatin carbo cis, or carbo plus gem versus Enfortumab vedotin + pembrolizumab, so most of the studies that are done are frontline. Have historically actually been done in a cisplatin ineligible population because of just the strong activity of cisplatin. So we’re gonna have to see what ends up happening with this, and this’ll absolutely change, how we treat patients with, urothelial cancer.
What’s unique about this study, however, I guess one of its pitfalls is, it was designed prior to, the approval. Zab in the maintenance setting post cis platin carboplatin. So this study doesn’t allow for maintenance maintenance checkpoint inhibition in the control arm. And so I think there’s always gonna be that outstanding question about what to do for those patients.
Trastuzumab Deruxtecan
But this is a very exciting combination regimen to look out for. All right, so then, Trastuzumab deruxtecan is an antibody drug conjugate that’s comprising an anti HER two antibody, a cleavable linker, and a a topoisomerase one inhibitor payload. And in a, Phase 1 trial of selected patients with urothelial cancer who are actually seeing.
Signal of activity, objective response rates of 37%. You can see the spider plots there demonstrating response. This is in a targeted population. So I think that her two targets in, bladder cancer is something to look out for. and, certainly potential for more personalizing care for patients with urothelial cancer.
And then I’ll highlight the data regarding Cabozantinib. I will invite Monty up here to give this talk, but give this portion of the talk, cuz I think he presented the data at ASCO last year. ,, the cosmic O two one study looked at Cabozantinib in combination with the Tocilizab, demonstrating modest activity.
You can see sort of this, this ineligible cohort there. Rate of around 20%. The CIS eligible response rate is around 30% of patients who’d received a prior checkpoint inhibitor response rate around 10%. There is a large cooperative group study called Main Cav being chaired by, Dr. Shepa Gupta, looking at adding Cabozantinib in the.
Setting, post a stable, progressive disease, or response to platinum-based chemotherapy. so that is an important trial that’ll answer an important question. And lastly, I’ll highlight N-803. And while this is an advanced, tor discussion, I think this, this agent is quite exciting. It’s, immune activating I L 15 superagonist.
And the data were presented at ASCO last year and are now published as well. demonstrating significant response rates. complete response. This is for a local non-muscle invasive bladder cancer cohort. A looked at patients who had evidence of, carcinoma and CSU demonstrating a complete or partial response, rate of 71% median duration of response.
Almost two years. And so this agent, I think, is currently under expedited review, by the FDA for, approval. This is an unmet need for people with persistent and recurrent cys, post, BCG or BCG unresponsive disease. It’s a real unmet. . All right. So that was sort of our whirlwind tour, with technical challenges of novel therapies in genitive urinary malignancies, this is just just a little color of the things that are out there. There’s a lot more cool drugs and agents to be looking out for. So many novel agents are currently in development across all genitive urinary malignancies. There’s a novel. There’s novel modes of drug delivery in RCC novel TKs.
Eyes and Strategies to target the VEGF H pathway are under development, and additional checkpoints are also being explored for prostate cancer. Continued targeting of the anti angio receptor, remains important for this disease. In addition to targeting novel, targeted therapy pathways such as AKT and CDK 4/6 and in urothelial.
Combination strategies of targeted therapy and immunotherapy are being explored. And additional novel intravesical therapies I think are something to look out for in the future. So, you know, it’s exciting to see the landscape continue to evolve, and I’ll take any questions like, share and subscribe here on OncologyTube. For notifications when similar videos are available.