


2023 ASH AML Updates [Slides] – Kiran Naqvi MD – MOASC
Acute myeloid leukemia updates from our recent ASH from 2022
By Kiran Naqvi, MD
Acute myeloid leukemia. These are the updates from our recent ASH from 2022 Acute myeloid leukemia. These are the updates from our recent ASH from 2022. So moving on. The first abstract that I wanted to talk about was an acute promyelocytic leukemia standard risk not high risk where patient, this is a Chinese study, sorry.
And. What they did was they compared ECTRA in combination with an oral formation of arsenic known as RGA Indigo. And this was a study which was a non-inferior trial where 81 patients with newly diagnosed standard risk APL were enrolled. 75 patients were treated. All of them got induction therapy with eight ATRA and IV arsenic trioxide.
And once they achieved cr, the consolidation, they were random. Either to receive an ATRA in combination with IV ATO O versus ATRA in combination with the algar indigo, the oral arsenic. And what they found was a hundred percent of the patients achieved a complete molecular response, meaning a PCR showing no evidence of translocation.
1517. By the end of the second cycle of consolidation, there were no relapses, no. And adverse events were very similar to oral arsenic and IV arsenic. Were not different. And if you look at this, Graph you can actually see then the event-free survival was a hundred percent between IV versus oral.
So this is an interesting study because, in patients with standard risk, a p l, after achieving cr, we give four cycles. It’s a monthly, four weeks on, four weeks off of IV arsenic trioxide. And if we can get an oral formulation, it might just work best for patients and easier for patients. The second study also from China what they did was they compared seven plus three with or without sorafenib and newly diagnosed core binding factor leukemia.
And I found this study interesting because, a lot of times we see patients with core binding factor leukemia, having. Either FLT3, three mutation, RAs mutations, or c-Kit, as we all know. And sorafenib is a multikinase inhibitor. It inhibits FLT3. It does inhibit c-kitt. So in this study, they had 64 patients randomized in a one-to-one fashion, got getting seven plus three with Orbita sorafenib in the induction cycle.
They got, gave 400 milligrams twice sorafenib for two weeks. And then in the consolidation cycle they gave 21 days instead of 14 days. And then the difference is patients who got randomized to the sorafenib arm also received maintenance sorafenib for 12 months. In terms of grade three to four adverse events, it wasn’t different.
But if you look at the responses, the CR rate was not different with the addition of sorafenib. However, what we they noted was that the, what they call the major molecular response, Meaning if you do up Q PCR for translocation, A 21 or inversion 16 and less, and the value of less than 0.1 was defined as MMR was superior or was higher in patients who got chemo with sorafenib.
The same thing with a complete molecular response, which they defined as a transitive level of less than 0.001. And this was the primary endpoint of the. That after cycle four of consolidation, what was the complete molecular response rate? And again, it was higher in sorafenib arm. So the question is, does sorafenib really improve outcome in core binding factor Leukemia is Why is, why do we see this is.
An effect of sorafenib on maybe FLT3 three mutated patients or cki, or it might be a non-specific effect of sorafenib that can also be happening. There are some angiogenic effects of sorafenib that we we know and there was a study, Cremel study, very popular from Germany, 25 centers, and they saw that irrespective of the FLT3 three.
Patients who got sorafenib still did better. But based on this study, we are still not like convinced that we should start treat our core binding factor leukemias with chemo plus sorafenib. But this is an interesting finding. . The next abstract was from MD Anderson. And this is a combination of CLIA along with Venetoclax in newly diagnosed AML.
So CLIA is actually clarien given for five days in combination with Cytarabine. The doses is 1.5 gram per meter square, five, five days along with idarubicin. And what they did is they all added ve. During the induction cycle for seven days, they started that from day two to day eight. These were younger patients and the median age was 48, up to the age of 65 years was allowed.
And if you look at the responses here, the CR rate with CLIA-Venetoclax was around 85%. And if you just compare it with seven plus three, it’s around, 50 to 60% in seven plus three. So it was 85%. And if you look at the MRD negativity, it was significantly high. 90% of the patients who achieved a CR also were negative by Mr.
A good number of patients. 62% of the patients actually proceeded to stem cell transplant. And the mortality, if you look at early mortality and eight week mortality was was acceptable. Here the two, your overall survival, if you look , I’m just trying to see this is the world survival here?
Yeah, it was around 71% and the event-free survival is 68%. And here it’s just a graph showing that patients who went to transplant, which is in the blue one, did better than patients who did not go for transplant. But if you look even at the patients who did not go for a transplant, I think they did tremendously well.
So do we transplant These patients are not, I it’s hard to say. Again, continuing on into the same study. They, this is by e L n, favorable, intermediate and Adverse Risk, and you can see that patient did in the favorable risk. This is their event-free survival compared to the orange curve, which is the intermediate risk.
Sorry. No, that’s the adverse one and the blue one is the intermediate. And this is the overall survival. So even by e ln, you can see that the patients who were in the favorable risk did really well with CLIA-venetoclax compared to those who were in the intermediate or adverse risk, is hard to say because they’re overlapping the intermediate and the high risk.
But I think we may just need longer follow up of the study. All right. . So this is the Jemima trial from Italy. Here they had Juanita Clax and what they did was they combined it with not similar to CLIA, but they used Fludarabine, the Fludarabine, idarubicin and Cytarabine. So in combination with Juanita Clax.
But what they did is the only included patients who were intermediate or high risk by ELN 2017. So they had a total of 57 patients. I would say younger age group who got Vela with F L A I, this is the dosing. What they also did is they tried to see if when 600 was better than when 400. So that’s the other thing they were trying to study in this in this in this trial.
So the CR rate was 70%. But with the mrd negativity of 74%, the two month mortality was 5.3. 49% of the patients went for ELO transplant in one year. Overall survival was around 76% or, and the median oral survival was not reached. And here are the results that you can see. But what they noted was there was no significant differences in safety cr neuro survival between the two windows doses.
So the recommendations are still to go with 400 milligrams and not 600 milligrams of venetoclax. , and you can see it right here. This is the disease-free survival probability. This is the arm that’s getting 600 and this is the arm that’s getting 400.
FLAG-IDA in younger, newly diagnosed AML patients
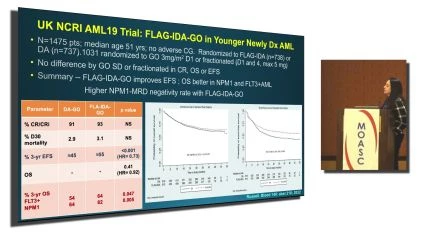
Trial out of uk. This was also, I thought was a very interesting trial because what they did is, this is the FLAG-IDA in younger, newly diagnosed AML patients. This so around 1500 patients, young, 51 years old, no adverse cytogenetics. These patients actually were randomized twice, were randomized to get FLAG-IDA versus Aubin Cytarabine, and then they added GO to these patients either at a dose of three milligrams perimeter square, standard dose on day one.
Or they fractionated it on days one and four, but the maximum was still five milligrams. And what they saw that. Standard dosing versus fractionated dosing of GO, GO didn’t make a difference. The CR overall survival in EFS was the same. How, and however, in FLAG-IDA GO versus idarubicin, the event-free survival was better with FLAG-IDA.
And here you can see the dotted line is FLAG-IDA versus this is the d r, the overall survival. Was not different here between the FLAG-IDA versus Uben and cytarabine. But what they saw that when they did a subgroup analysis of patients who were FLT3 three mutated or NPM unmutated, that seems to be an improvement in patients who got FLAG-IDA.
They, their overall survival was 64% versus 54 and fifth three mutated AML and 82 versus 64 and npm mutt. AML. So even though the overall survival was not different overall in the patients, but in the subgroup analysis they showed that patients who were FLT3 three positive and NPM one positive, they benefited with getting FLAG-IDA plus G compared to Duru and a c g.
So here is where the event-free survival from the same trial. As I said, patients who Gowan Rubicon a c were inferior to those who got FLAG-IDA. And this is the event-Free Survival where, which really shows that patients who got fractionated GO here, GO one g. It’s basically GO. One is the standard in G2 is the fractionated.
There was no difference. So here the FLAG-IDA plus GO, and this is Duwan Ruben, a c g, but there was no difference in terms of standard administration versus fractionated.
then. This was a study where they were, they were trying to study check chemotherapy with or without go in NPM one, mutated acute myeloid leukemia. This was a phase three study and 588 patients were randomized to receive intensive chemo. This is a rine study, so they’re giving three plus seven with atopic side.
With atra. So this is something that’s still being used in Europe with or without GO. And the dose of GO was the standard GO dose, three milligrams per meter square in day one. Median age was 58 years, and what they saw was that there was no difference in overall survival, irrespective of GO.
So the oral survival was not different, and there was an improved trend in the event. Three survival in patients who got the go. However, what they noted was, Event survival and the cumulative incidence of relapse was better in patients who got GO and were young. So in younger patients, GO seems to be working doing some good for the patients who are NPM mutated.
We didn’t see the same effect in patients who are older.
Watch and Share the Video Interview Here: https://oncologytube.com/v/41754
This study is out of Fred Hutch.
This study is out of Fred Hutch. Dr. Eli Estee, who passed away a year ago. He was working on the study where they were doing clam in combination with sorafenib in newly diagnosed AML and also high-risk MDs patients. This is a phase two study where 61 patients were a received clg m in combination with sra.
A dose of 400 milligrams twice a day. And then 71 patients got CLA GAM alone. Again, young population, 50 years. Since they’re getting chemotherapy, there was no difference in either the CR rates or the response rate. MRD rate, survival rate. With or without sorafenib. And here are the responses in the C clam arm and the C clam sorafenib.
So you can see there was basically no difference. These are the P-value. However, what they found was that if you go by e ln, the patients who were in the intermediate risk group, They had a longer overall event and event-free survival by ELN 2017. Intermediate risk. Can this be the effect of FLT3 three? Because a good number of patients who are an intermediate risk, EL LN 2017, their FLT3 three positive, can this be an impact of sorafenib on those patients?
But that’s what it showed in other, in favorable risk as well as in adverse risk. Eln, this effect was not.
The next study was was seven plus three. With 60 versus 90 milligrams of Duwan Rubin for newly diagnosed patients. And so the aim of this particular study of was first was 60 sufficient versus 90. And then in this study they were also trying to see if patients who responded, Two therapy induction, chemotherapy and had a bone marrow and day 15 with a blast showing under 5%.
Was there any benefit of giving them a second induction cycle or should we just proceed with consolidation? So 864 patients got three plus seven. There were randomized to 60 or 90. A standard for three days. This was the median age, but after 200 and patient 18 patients were enrolled on the study.
What they found was that the overall response rate with Duwan Rubus in 60 was 42%, and Duwan Rubus in 90 was 49, very similar. So then they stopped and they just enrolled all the remaining cohort on Duru and 60 M. And what they also saw that in patients who responded with less than 5% last after the first induction cycle, there was no benefit in the relapse free survival or overall survival if you gave them a second induction cycle.
So there was no benefit of giving them a second induction if they responded with the first induction. So this is the survival curve overall survival of Wan Rubus in 60 versus 90. You can see there’s an overlap. The Azacitidine rd ratio is 1.19 and this is the survival probability. If you give one induction versus double induction.
Again, the curves are pretty much overlapping. Okay. And then very famous y l study that got approval of Azacitidine in patients with newly diagnosed acute myeloid leukemia who were otherwise ineligible for intensive chemotherapy. This is just this is a three year follow up actually, and so 431 patients we all know, randomized in a two and two one fashion to get Azacitidine when versus Azacitidine alone.
So what they found as of this, the presentation when they did, out of the 286 patients, you can see Pat 11 patients had progressive disease in the Azacitidine, an arm while in the placebo Azacitidine. The progression was higher of 14.5% 14.5%. Again, treatment failure was higher in Azacitidine placebo arm, and the mortality was also seen to be higher in the Azacitidine alone arm versus Azacitidine.
These are the adverse events between Azacitidine and placebo Azacitidine, but what they, there were no new safety signals. Basically, that’s what it was. There was no new safety signals compared to when they presented the data with 75% os.
So here’s the duration of CR and c r i at a median follow-up of around 43.2 months. And you can see these two curves of Ben Azacitidine here versus placebo Azacitidine. The median duration is of Azacitidine of C R I with Azacitidine. VE is around 18 months and around 11 months with placebo is alone. But if you look at the median oral survival, we still see that the median oral survival with a.
14.7 compared to Azacitidine alone, which is 9.6. But what is really worrisome to me is that, we still have not hit a plateau. We are, the curve is coming down. So is it still, do we still believe that HMA van is optimal or is it suboptimal because the curve is still down trending? So I’m hoping with longer follow up, we’ll get more information.
but this remains the standard of care for our elderly patients, ineligible for intensive therapy. . Then this is another clinical trial, which I, it’s interesting because I use this quite a bit in my practice in my elderly patients with Cladribine low dose cytarabine. This was a trial, this was a combination that was quite often used in patients where, who were elderly in newly diagnosed AML at MD Anderson.
This was prior to Azacitidine when being the standard of care. And what they did at MD Anderson is that they added venetoclax to this combination. So they had 93 patients. These were elderly patients, age 68 years, where they gave cladribine for five days at five milligrams per meter square. And the low dose RSC was 20 milligrams twice a day.
and it was like two cycles of Cladribine LO dose, a C when alternating with Azacitidine. We, and the first cycle when was given for 21 days during induction and then consolidation, obviously the dose was reduced and treatment was allowed for two years. And if you see here the CR rate in this elderly population with Claine, Lowes, like 78% with a composite CR rate of 92% in MRD negativity of 81%, which I think it’s.
It’s really good. Early mortality, 2%. And then the overall survival is still at, I think, pretty decent at 68%. And some of the patients were still able to go to transplant, like 41%. And patients who did go to transplant, you can see the blue CLIAr curve here. They did better than patients who did not go to transplant.
And here’s the median overall survival at 12 months of 76% and at at two years at 68. . And and so this is also an important study. I know there’s a lot of talk about how to treat these FLT3 three mutated AML patients and gilteritinib being a great drug because it inhibits both the I T D and the tkd.
So this also is a study out of MD Anderson’s the phase one two study where they studied a triple combination of Azacitidine vain gilteritinib in patients who were three mutated where. 47 patients treated 27 were nugi diagnosed, 20 were relapsed refractory. And this is the dosing of the gilteritinib. They actually started off with Gil 80 and one 20, and I think they had six patients enrolled at in Gil 80 milligram arm.
And then I think four in one 20. But the recommended phase two dose was 80 milligrams of gilteritinib in combination with Azacitidine. . And in the frontline cohort, if you see, the frontline cohort has, does great. The the modified CR C is like a hundred percent. All the patients responded 92% with the CR four.
With the CR I, there were some ml fs, morphologic, leukemia free straight patients, but the relapse refractory arm I don’t think it did as well. So don’t know if we have patients who have Azacitidine and then we should add gilteritinib. , I don’t know how much benefit, but still I think it’s, I think it’s still okay to add Gilteritinib in our relapse refractory setting through Azacitidine.
So this is the relapsed in overall survival in the frontline cohort with the median follow up of 12 months. You can see here that the one year relapse three survival is 74% while at one year overall survival when the frontline cohort is 85%, which is phenomenal. Infant three mutated AML. In the relapse refractory cohort obviously not as good.
Only 25 with relapse-free survival at one year and in a one at one year. The overall survival is 30%. Okay. All right, and so this is Azacitidine when Mero, this is a star drug right now. We are trying, a lot of studies are ongoing. This is the NT CD 47. It’s being studied in MDs NTP 53 mutated AML. Then there is an enhanced two study and an enhanced two three study where they are studying the combination of Azacitidine when MA or Azacitidine MA alone in newly diagnosed patients.
But this is a study out of MD Anderson, phase one, two. 43 patients with newly diagnosed AML. 33 with de novo and 10 with secondary. And what I just wanted to focus here is the responses in the TP 53 mutated patients with Azacitidine and macro. The overall, the CR rate is 46 in the mutated, which is, I think it’s really good because we don’t really have a good drug to target the TP 53 mutated patients and the MRD negativity is it’s pretty significant.
64%. So overall the Mali seems to be working in this t in this poor population of patients where, we are seeing some good responses. And you can see here the mortality with this combination is zero. At four and eight week.
And so this is again, the duration of response in of overall survival in the frontline cohort. Duration of response is at 16, 18 months, 52%. The TP 53 mutated, and 74% in the vial type. And here are the overall survival. Obviously, TP 53 valve types, they do better than TP 53 mutated, but still the 12 year month oral survival is 53.
And the other thing that MD Anderson did is that they compared the Azacitidine MA study to the historical h HMA van combination that they did in TP 53 patients mutated patients. And because and they over there, they use Azacitidine or DEC 10 days with Venetoclax. And what they found was that patients who got Azacitidine TP 53 mutated versus HMA Ven, TP 53 mutated, the survival was better.
The macro arm.
And so this is and again, coming to this is the relapse refractory study where they used Venetoclax in combination with FLAG-IDA v this combination we often use in patients also in frontline, but in the relapse refractory setting. I just wanted to show you that a combination of FLAG-IDA with venito.
In 33 patients with relapse refractory AML, the overall response rate was 61% and the CR rate was 40%. MRD negativity was 40. So in a relapse refractory setting in AML, achieving a CR rate of 40% in MRD negativity of 40, it’s pretty good. And in reducing this, think this regimen in patients 42% of the patients were still able to go to stem cell transplant.
And again, moving on to the same study this is just the overall survival and the duration of response. You can see that the median oral survival in this really relapse refractory setting was 17 months and one year overall survival of 56%. And this is the duration of response of 33 months. So I think and this, these are not patients.
I don’t believe that these are the patients who went to transplant. These are patients who strictly got FLA IDA treatment in relapse refractory. And then really quickly, this moving on to some of the targeted therapies that were being studied in AML. This is PAB Crine. This is an Im GN 6 32 study.
Dr. Gia Kumar is also part of this study. Correct. So it is a combination of I Amgen 6 32. This is antibody, which is targeting the CD 1 23 protein expression on the AML cells in combination with Azacitidine and Venetoclax, such the triple therapy in high risk patients relapse refractory. And I just wanted to show you that these are patients who are relapsed refractory, have also received prior transplant, prior when and in the I T T population.
Of the 91 patients who are enrolled, the response rates are pretty, are still pretty good, 45% and a CR rate of, it’s not good of a CR rate, but the composite CR rate is still like 25%. A good number of patients probably ha are getting their bone marrow emptied and hopefully maybe these patients can proceed to trans.
So this is a study which is still ongoing. Hopefully we’ll hear about it more in the upcoming congresses. And then this is the menon inhibitors. Men inhibitors are on the rise right now to target the m l gene rearrangement and the also have shown some activity in NPM mutated AML. So this is revumenib as a SNDX 5613 study one drug where 60 patients relapsed refractory AML, who were KMT to a rearranged m mlg rearranged or had NPM one mutation.
And these are the responses. You can see that the responses overall, In these high risk patients, at least the ML L is high risk was 53% overall response rate, MRD negativity rate of 56%. And if you go with the subgroup analysis, you can see that the world response rate in a relapse refractory setting was 59% in rearranged patients AML.
And in npm one was 14 was 36. . So these are some newer drugs that we, they’re studying in patients with MLL gene rearrangement. And this is also another drug MLL gene rearrangement by Dr. Herba from Duke. And so this is another drug Z Toink active against mll as well as NPM one. So here are 58 patients with relapse refractory AML 55 had KMT two.
And 45% were NPM one mutated. And in the phase one study they studied a dose between 50 to a thousand milligrams. And then they decided that they would be in a phase one B study. They will explore 200 versus 600, and they found more activity with the 600 milligram dose. And so now in the phase two study, they’re expending the 600 milligram dose.
But you can see there is, of the 18 patients there. Some activity in the ML L gene rearrangement, but definitely in npm unmutated patients the overall response rate is 40%. So it’s pretty. . And these are just my last few slides. This is one drug that I just wanted to mention because it was just recently approved on December 1st by the fda.
This is FT 2 1 0 2 olutasidenib. This is an IDH one inhibitor, and this was approved in the relapse refractory setting and patients who harbor in IDH one are 1 32. Mutation and these patients had not received prior Ivo sittin. So these were IDH one naive patients, and they got the drug at a dose of 150 milligrams twice a day.
And in the relapse refractory setting, the responses were the C R H was like 35%. And the, the duration of response was was decent around two. and these were patients who also had received Venetoclax because we know that Venetoclax has activity in IDH mutated patients and even in patients who received prior, when the response rates were very much similar.
In terms of side effects, like other IDH inhibitors, it does cause differentiation syndrome seen was seen in 14% of the patients. , but pretty manageable by steroids and hydria. So not a problem. So here are just the responses, and this is just the survival by response here. And last, this is my last slide.
I just thought this was also an interesting study because we often talk about CHIP in AML and we talk about DN MT three A mutations and tech two mutations as well as XL one. And oftentimes we treat the patients and we do an n. An ngs and we still see DTA mutations existing. And so we are like, oh, this is chip.
So this particular study was trying to see if there was any prognostic significance of persistence of these mutations. So they had 189 patients who were treated with on, on this trial, alpha 0 7 0 2 study. So they got intensive chemotherapy, 189 patients, cr, the chief CR of those 90 patients were tested positive.
By M R d ngs, M r d and 42 of these ngs, m r d actually harbored the dta mutations only. So they only had these, so they didn’t have any of the bad, the other ones, patients of 46 years of age, the. Leukemia fee Survival who harbored the DTA was 35 months and the overall survival was 41 months.
There was no significant difference in patients if they had Mr. D of the DTA mutations versus the non DTA mutations. So here you can see the curve, R D ngs, the top one. Yes, patients who are negative by ngs. And then the middle curve is those who actually had DTA at the end of the induction cycle.
And then these are patients who had non DTA mutations. So what I’m trying to get on through this study is that patients who continue to, Have the DN MP three A attack two, and as SX and mutations after induction therapy. Maybe we just didn’t, we cannot just blame it being on chip and then we expect them to do okay.
I think these patients still do not as good as who are MRD negative by D nng. S Sorry, ngs, say that again. You witnessed before the, so they were positive before the ngs, and then they got induction, and then they still had persistence. So the question was, oh, these are chip mutations. What do we do? We just watch them, but we see that the persistence is not as good as them being negative.
All right, so I’m sorry I went through a lot of these abstracts, but please feel free to reach out to me if you have any questions. This is my email. This is my personal cell, and I’m happy to take any questions.
About The Author:
Kiran Naqvi MD –
Hematologic oncologist Dr. Kiran Naqvi is a board-certified physician at UCI Health. Her clinical interests include bone marrow aspiration, bone marrow transplantation, myelodysplastic syndrome, chronic myelogenous leukemia, and acute myeloid leukemia.
She received her medical training from Pakistan’s Dow University of Health Sciences in Karachi. Following fellowships in hematology-oncology at Baylor College of Medicine and the University of Texas MD Anderson Cancer Center, both in Houston, Texas, she completed a residency in internal medicine at the University of Illinois Urbana-Champaign and the Carle Foundation Hospital in Urbana, Illinois.